
Eye Diseases
Our top priority is the care of your eyes. We want to keep your eyes healthy through regular eye health evaluations, communication, and education. This page lists a few of the most common eye diseases. Select from the following list of topics or scroll to learn about the causes, symptoms, and treatments for:
Blepharitis


There are two types of blepharitis. Seborrheic blepharitis is often part of an overall skin condition called seborrhea, which may also affect the scalp, chest, back and the area behind the ears. The second form of blepharitis – staph blepharitis – is a more severe condition, caused by bacteria, that begins in childhood and may continue through adulthood.
Causes
Hormones, nutrition, general physical condition, and even stress may contribute to seborrheic blepharitis. Build-ups of naturally occurring bacteria contribute to staph blepharitis.
Symptoms
Blepharitis could be described as dandruff of the eyelids. Seborrheic blepharitis results in redness of the eyelids, flaking and scaling of eyelashes, and greasy, waxy scales caused by abnormal tear production. Staph blepharitis can cause small ulcers, loss of eyelashes, eyelid scarring, and even red eye.
Treatment
Careful cleaning of the eyelids can reduce seborrheic blepharitis. Application of hot packs to the eyes for 20 minutes a day can also help. Staph blepharitis may require antibiotic drops and ointments.
Cataracts
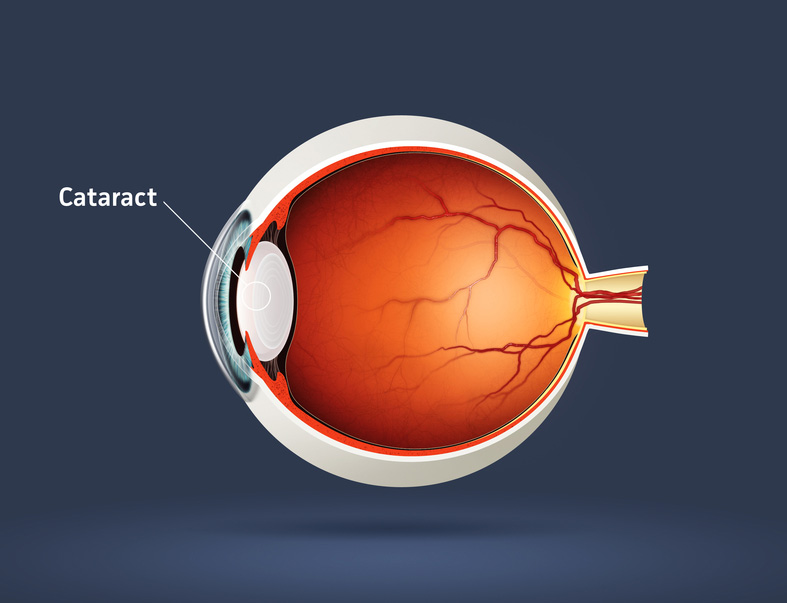

A cataract is an opacity of the lens of the eye. The body's natural lens is similar to an onion, with many layers. These layers contain protein and as the proteins clump together, they cover the lens and make it difficult to see clearly. Cataracts are generally seen in the older population, but they can occur at any age, even birth. By age 60, over half of the population has some symptoms of cataracts due to the natural aging process.
Cataracts are painless but if left untreated can lead to blindness. Cataract surgery is done on an outpatient basis with little or no downtime afterwards. The surgery is performed by a medical doctor known as an ophthalmologist, who specializes in surgery of the eye. The aftercare or postoperative care can be administered by an ophthalmologist or an optometrist.
Symptoms of Cataracts
There can be a myriad of symptoms when a person develops a cataract. It is common for vision to be blurry, as though you are looking through a foggy window. Color vision changes occur in which the brightness of colors fade, especially blue and green. Patients with cataracts also experience difficulty in reading small print. They also feel like they need brighter light or possibly a new glasses prescription. Double vision or vision that seems like halos around the letters also occurs, as well as sensitivity to light.
Causes of Cataracts
The exact physiological cause of cataracts is unknown, but there are many risk factors. Aging and trauma are known to cause cataracts. A blunt trauma or injury to the eye can cause a cataract at any age. The effect of aging on the cells of the lens contributes to cataracts usually after age 60. There is also a direct correlation between the sun's UV rays and certain radiation exposures that contriibute to cataract growth. Smoking is a big risk factor for developing cataracts as well.
Poor nutrition can add to the risk of developing cataracts. Lack of vitamin C has been shown to increase the genesis of cataract formation. Some prescription medicines, especially prednisone, can cause cataracts. Diabetes and other chronic disease processes are also factors in cataract formation. Finally, there are genetic factors that contribute to a cataract.
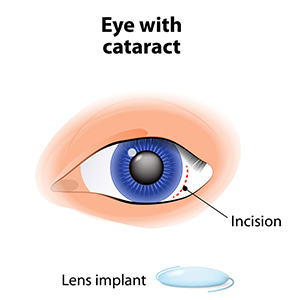
Treatment of Cataracts
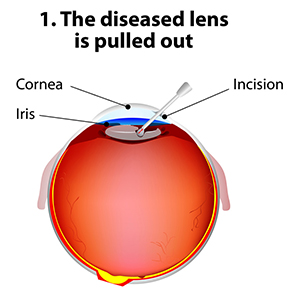
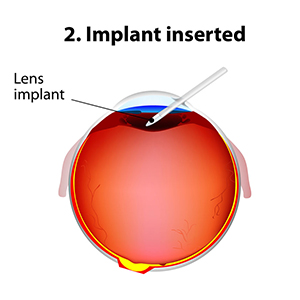
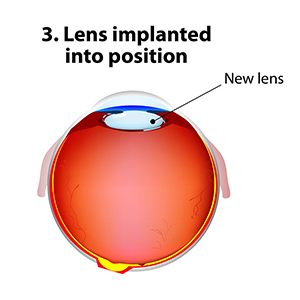
The standard of care for the treatment of cataracts is typically surgery. Cataract surgery, which is an outpatient procedure, removes the protein accumulation from the eye by replacing the cloudy natural lens with an artificial lens. This artificial lens, known as an IOL or intraocular lens, will have your prescription, which in most cases, makes you less dependent on glasses. Lens technology has evolved over the years to also accommodate prescriptions for astigmatism and bifocal prescriptions. Cataract surgery is one of the most commonly performed surgeries in the United States, and it has a success rate of over 98%.
There are many types of cataracts that form on the eye, with different levels of density. This can affect the post-operative care of cataract patients. After cataract surgery, it might be necessary to use a laser to clear an after-cataract membrane that can occur weeks to months after the procedure. This treatment uses a YAG laser and is a painless, low risk, in-office procedure. Most patients can return to work or normal activities within days after the procedure. Your doctor will likely prescribe eyedrops to prevent infection and swelling.
Recent Findings
New technology in cataract surgery includes a bladeless customized procedure that allows for faster healing and clearer vision after the procedure. This computer assisted surgery uses a laser to make the incisions. The laser also divides the cataract efficiently so that the surgeon can remove the old lens and replace it with a new state-of-the-art IOL ( Intraocular lens). This technology uses a femtosecond laser which emits cool pulses of energy. This technology has been used for decades in LASIK surgery for the correction of myopia or nearsightedness. This form of cataract surgery now allows the procedure to be more precise, and reproducible.
Citations
1. What is a cataract? Educational website release. Triadeye.com. January 13, 2013.
2.Bladeless cataract laser surgery. LenSX press release. October 4, 2012.
Conjunctivitis

Conjunctivitis, commonly called pink eye, is a redness of the eye. It is often accompanied by a discharge (clear, yellow, or white) and itching in the eye.
Causes
Pink eye is most often a viral infection, but it can also be caused by bacteria or an allergic reaction. Viral pink eye is highly contagious.
Prevention and Treatment
To avoid spreading conjunctivitis, wash your hands often, do not touch the infected area with your hands, do not share washcloths or towels, and avoid using makeup which may become contaminated. A child with pink eye should be kept from school for a few days. Sometimes an eye doctor will need to prescribe antibiotic eye drops and ointments to clear up conjunctivitis.
Diabetic Retinopathy
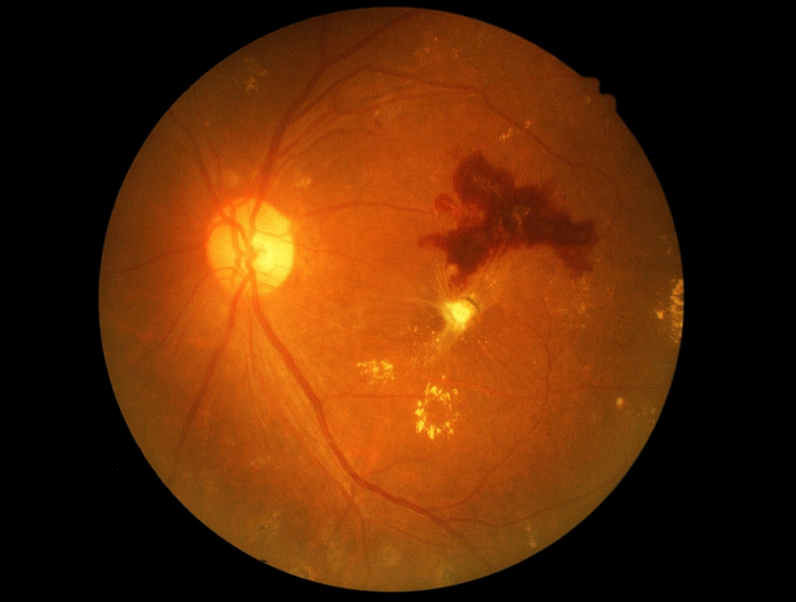

Diabetic retinopathy is a condition associated with diabetes. High levels of blood sugar may damage tiny blood vessels in your eye. New vessels may form to replace the damaged vessels. The new vessels can burst, resulting in blurred vision or even blindness.
Symptoms
Symptoms of diabetic retinopathy include:
- "Floaters” – small specks that pass across your field of vision, made up of cells floating in the transparent gel of your eyeball
- Difficulty reading or seeing things close-up
- Sudden loss of vision
- Flashes
- Blurred or darkened vision
Risk Factors and Treatment
If you have diabetes, make sure you control your blood sugar level. This will reduce your risk of getting diabetic retinopathy. If you are experiencing some of the symptoms listed above, give us a call. If diagnosed properly, diabetic retinopathy can be treated with a laser procedure or a vitrectomy.
Dry Eye Syndrome


If your eyes are constantly itchy or dry, you may have dry eye syndrome, which affects many millions of Americans. Dry eye syndrome is caused by a lack of, or poor quality of, tears. Tears lubricate the outer layer of the eye called the cornea. If the tears are not adequate or are not composed of a proper balance of mucous, water, and oil, the eye becomes irritated.
Symptoms
Dry eye syndrome leads to a number of symptoms, including itchiness, irritation, burning, excessive tearing, redness, blurred vision that improves with blinking, and discomfort after long periods of watching television, using a computer, or reading.
Risk Factors
There are many factors that can contribute to dry eye syndrome. These include dry, hot, or windy climates; high altitudes; air-conditioned rooms; and cigarette smoke. Contact lens wearers, people with abnormally dry skin, and the elderly are more likely to develop dry eye syndrome. You may also be more at risk if you take certain medications, have a thyroid condition, a vitamin-A deficiency, Parkinson’s or Sjorgen’s disease, or if you are a woman going through menopause.
Eye Allergies
 Red, watery, itchy eyes are a common problem in Prescott. Many times, the culprit is seasonal allergies, that also cause symptoms of sneezing, nasal congestion, and a runny nose.
Red, watery, itchy eyes are a common problem in Prescott. Many times, the culprit is seasonal allergies, that also cause symptoms of sneezing, nasal congestion, and a runny nose.
Causes
Trees such as juniper and cottonwood, weeds, grasses, etc. can all be contributors. Sensitivity to cosmetics, lotion, soap, cologne, perfume, etc. may also cause eye allergies.
Symptoms
Eye allergy symptoms may range from mild itching to severe redness and swelling of the conjunctiva (the mucous membrane lining the eyelids and on the surface of the white of the eye) and swelling of the eyelid skin and the skin surrounding the eyes.
Treatment
Palliative treatment such as cool compresses and a good quality artificial tear to rinse the ocular surface may be enough to relieve symptoms. An over the counter allergy eye drop may be a good next step, however, some may do more harm than good. For instance, some may perpetuate a cycle of eye redness by use of a short-acting vasoconstrictor that results in a larger re-dilation of blood vessels when it wears off. Our office can provide specific recommendations for OTC drops based on your clinical appearance. Sometimes, eye allergies can be severe, and a prescription eye drop or topical cream for the skin around the eyes is required.
If you feel you have an eye allergy that needs attention, please call us for an appointment. We will do our best to accommodate seeing you, many times on the same day!
Floaters (Vitreous Degeneration)
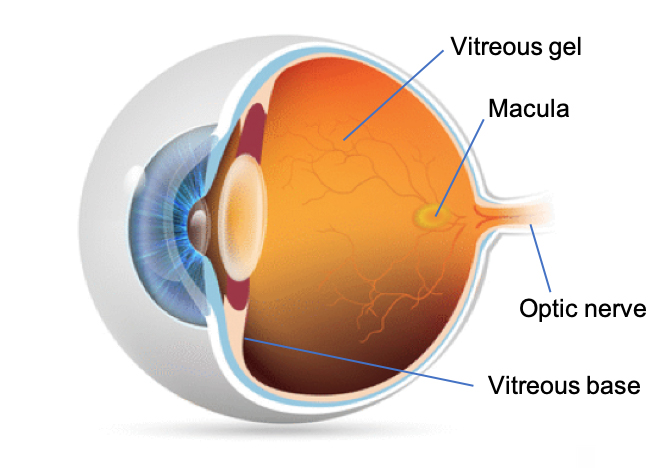 The vitreous is a gel-like substance that fills the posterior cavity of the eye. The outer surface of the gel contains millions of tiny fibers that tightly adhere to the vitreous base anteriorly, and with a less tight adherence to the retina and optic nerve posteriorly. As we age, the gel starts to shrink, the fibers break, and the gel pulls away from the retina causing floaters. When you see floaters, you are not actually ‘seeing’ them. You are seeing the shadow of the floaters. Therefore, you will notice floaters more in bright sunshine than in a dimly lit room.
The vitreous is a gel-like substance that fills the posterior cavity of the eye. The outer surface of the gel contains millions of tiny fibers that tightly adhere to the vitreous base anteriorly, and with a less tight adherence to the retina and optic nerve posteriorly. As we age, the gel starts to shrink, the fibers break, and the gel pulls away from the retina causing floaters. When you see floaters, you are not actually ‘seeing’ them. You are seeing the shadow of the floaters. Therefore, you will notice floaters more in bright sunshine than in a dimly lit room.
Posterior Vitreous Detachment (PVD)
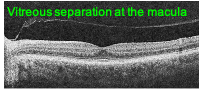 As the gel continues to shrink and pull away from the retina, one may notice a sudden increase in floaters or what appears as cobwebs in their vision. This may indicate that the vitreous has more fully separated from the retina and optic nerve as seen in the OCT photo to the right. Note the line above the retinal cross section, that is the vitreous face. In fact, an annular ring may be noticed along with floaters signifying the vitreous detachment form the optic nerve. Flashes of light that look like lightening streaks may also appear in your peripheral vision as the gel detaches and tugs on the retina.
As the gel continues to shrink and pull away from the retina, one may notice a sudden increase in floaters or what appears as cobwebs in their vision. This may indicate that the vitreous has more fully separated from the retina and optic nerve as seen in the OCT photo to the right. Note the line above the retinal cross section, that is the vitreous face. In fact, an annular ring may be noticed along with floaters signifying the vitreous detachment form the optic nerve. Flashes of light that look like lightening streaks may also appear in your peripheral vision as the gel detaches and tugs on the retina.
PVD complications
Fortunately, eighty-five to ninety percent of PVDs do not result in any harm; PVD is a natural occurrence with age. However, sometimes problems do occur. First, as the fibrils pull at the vitreous base, if they don’t break, it can cause a tear in the retina. Fortunately, retinal tears can usually be treated quite easily, but time is of the essence. The sooner a retinal tear is treated, the less likely it will progress to a retinal detachment. While a retinal detachment can also be treated, the risk of vision loss is higher.
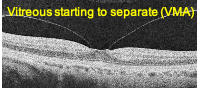 Second, the vitreous may incompletely detach from the retina posteriorly at the macula, leading to a condition known as vitreomacular adhesion (VMA). As can be seen from the OCT image on the right, a small amount of VMA may occur in early stages of PVD. The majority of the time this leads to a complete separation with no further visual consequences.
Second, the vitreous may incompletely detach from the retina posteriorly at the macula, leading to a condition known as vitreomacular adhesion (VMA). As can be seen from the OCT image on the right, a small amount of VMA may occur in early stages of PVD. The majority of the time this leads to a complete separation with no further visual consequences.
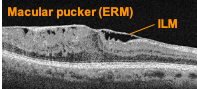 Third, sometimes as the gel separates, the vitreal fibrils don’t release easily and tug on their retinal attachment points over the macula. This leads to a wrinkling of the surface of macula, sometimes referred to as a macular pucker. A more formal name for this condition is Epiretinal membrane (ERM). The internal limiting membrane (ILM) is the outermost layer of the retina. As the fibrils pull on the ILM, it wrinkles and separates from the retina, henceforth being called an ERM. If the ERM significantly distorts vision, surgical repair is required.
Third, sometimes as the gel separates, the vitreal fibrils don’t release easily and tug on their retinal attachment points over the macula. This leads to a wrinkling of the surface of macula, sometimes referred to as a macular pucker. A more formal name for this condition is Epiretinal membrane (ERM). The internal limiting membrane (ILM) is the outermost layer of the retina. As the fibrils pull on the ILM, it wrinkles and separates from the retina, henceforth being called an ERM. If the ERM significantly distorts vision, surgical repair is required.
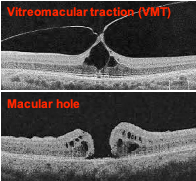 Fourth, the vitreal fibers may be more firmly attached at the macula leading to vitreomacular traction (VMT). VMT may cause visual distortion, such as a doorframe looking like it is bent. VMT is a more worrisome condition because if the vitreous and retina do not separate, the VMT can cause a macular hole. A sudden symptom of a dark spot in the center of vision may indicate a macular hole has formed. Macular holes must be surgically repaired.
Fourth, the vitreal fibers may be more firmly attached at the macula leading to vitreomacular traction (VMT). VMT may cause visual distortion, such as a doorframe looking like it is bent. VMT is a more worrisome condition because if the vitreous and retina do not separate, the VMT can cause a macular hole. A sudden symptom of a dark spot in the center of vision may indicate a macular hole has formed. Macular holes must be surgically repaired.
Get Evaluated!

Glaucoma
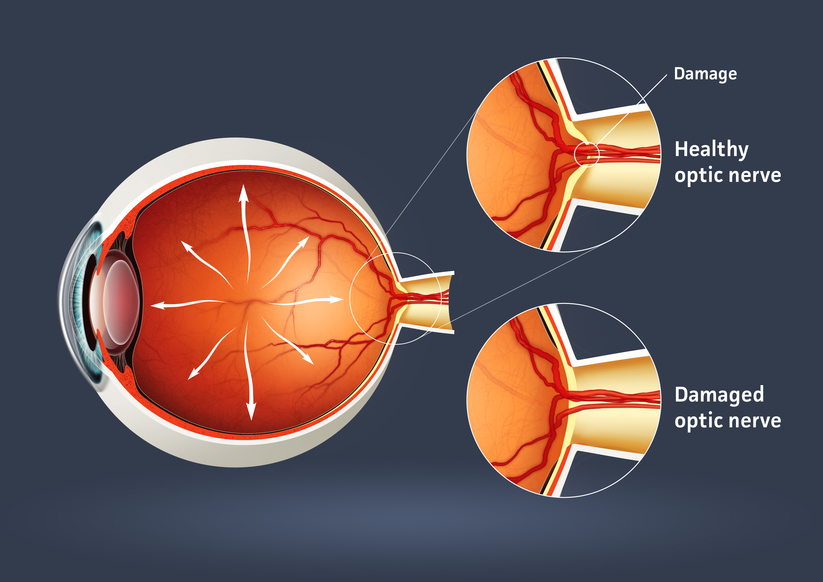

Glaucoma is a serious sight-threatening condition in which there is an abnormal pressure inside the eye. Typically, the pressure or IOP (intraocular pressure) is too high for the blood vessels and optic nerve to function normally, leading to loss of vision.
There are some forms of glaucoma that can occur with normal pressure in the eye. The average IOP for a healthy eye is 10 to 22 mm of Mercury. Just as a physician’s office tests your blood pressure annually, the eye doctor tests your IOP during annual eye examinations.
Types of Glaucoma
There are several varieties of the disease, with primary open-angle glaucoma being the most common. Primary open-angle glaucoma (POAG) occurs when the IOP is higher than normal. As the pressure increases, it destroys vital nerve tissue that is irreparable. POAG usually occurs over a long period of time, months to years, and slowly causes peripheral visual field loss. If left untreated, a sufferer progresses to tunnel vision and then to total blindness.
A second type of glaucoma is acute-angle closure. This is considered a medical emergency because the interocular pressure spikes suddenly to anywhere from 30-70 mm or higher. This causes extremely sharp pain, nausea and vomiting, and cloudy vision. The IOP needs to be lowered within hours to prevent permanent vision loss.
Juvenile open-angle glaucoma, or JOAP, is similar to POAG, in that is causes a gradual visual field loss. The most common form is in children from ages 3 to 21. Infantile or congenital glaucoma is a type of glaucoma that manifests itself between birth to 3 years of age. A typical sign is an enlarged bluish-gray cornea, the front dome of the eye. Excessive tearing of the eye and sensitivity to light are also symptoms. Finally, secondary glaucoma is caused from trauma, eye disease, or certain medications.
Causes of Glaucoma
Many theories on the cause of glaucoma exist, but the exact cause is unknown. Glaucoma can be a hereditary condition. It also can be caused by malformed anatomical structures in the eye. Certain risk factors such as hyperopia and cataracts cause a higher incidence of certain types of glaucoma.
One cause of glaucoma is an insufficient drainage system of the aqueous fluid. The aqueous imbalance causes a gradual buildup of pressure which destroys vision. Another cause is an insufficient flow of blood to the optic nerve. Ocular trauma or injury that damages the anterior segment for the lens and drainage mechanism of the eye can also lead to glaucoma. In the case of normal tension glaucoma, pressure readings are in the normal range. The cause of this is unknown.
Treatment
Even though in most cases there is no way to prevent glaucoma, there are many treatment options. Medications in the form of eyedrops are commonly prescribed. Different combinations of agents act on mechanisms of action to lower IOP or to slow the production of fluid.
Advanced surgical and laser procedures can also be viable options for the treatment of glaucoma. An in-office procedure called laser trabeculoplasty can cause the meshwork in the eye to work more efficiently. This treatment has a temporary effect and may need to be done multiple times. Another effective surgery uses a drainage implant to facilitate better outflow and inflow of aqueous fluid in the eye. These procedures help keep the pressure stabilized. Conventional surgery for glaucoma is done in an operating room scenario. A flap in the eye is created to facilitate outflow of the pressure. This pressure-controlling surgery is known as a trabeculotomy.
Furthermore, some oral medications can also be used in the treatment of glaucoma.
Methods of Testing for Glaucoma
During a comprehensive eye examination, eye pressure can be tested through various methods. Tonometry gives a pressure reading of the eye. A tomometer has different methods such as a probe that gently touches the front of the eye after the eye doctor has administered anesthetic eyedrops. Another method of testing uses a puff of air. For children, there is a tonometer that is quick and does not require anesthesia.
A pachometer, which measures the thickness of the front of the eye called the cornea, can also aid in diagnosis. A visual field device can measure for early or late damage in the peripheral fields of vision. Lastly, newer technology called OCT, or optical coherence tomography, counts the nerve fibers, which can help detect early changes in the disease.
Prevalence of Glaucoma
There are approximately 3 million individuals in the United States with glaucoma. It is the second leading cause of blindness in the country. Most cases are found in the population over age 40, and more women than men have the disease. Two thirds of glaucoma cases are in the Caucasian population, approximately 20% are African-American, and 10% are Hispanic. Glaucoma continues to rise every year in the population.
The key to success in the treatment of glaucoma is early detection and progressive monitoring of the condition. Comprehensive eye examinations and diligent monitoring will help protect from vision loss with this disease.
Citations
- Glaucoma. AOA pdf. AOA.org.
- I Care Tonometry in Children. JAAPOS. Sciencedirect.com. April 2011
- Glaucoma, open -angle. NEI source press release. 2010.
Macular Degeneration


Macular degeneration is a disease which affects a small area of the retina known as the macula. The macula is a specialized spot on the retina that allows us to see the fine detail of whatever is directly in front of us. Macular degeneration occurs when the macula begins to deteriorate.
“Wet” vs. “Dry”
Most often, macular degeneration is accompanied by formation of yellow deposits, called “drusen,” under the macula, which dry out or thin the macula. This is called “dry” macular degeneration. In rare cases, abnormal blood vessels develop under the macula and leak fluid. This is called “wet” macular degeneration.
Causes
A number of uncontrollable factors contribute to macular degeneration, including age, sex, eye color, farsightedness, and race. Risk factors you can control include smoking, high blood pressure, exposure to harmful sunlight, and diet.
Symptoms
It is difficult to detect dry macular degeneration in its early stages. The most common symptoms, when detected, include a spot of blurry vision, dark vision, or distorted vision. Wet macular degeneration progresses much faster than the dry variety. Both forms of macular degeneration can cause blindness.
Treatment
Currently, there is no cure for macular degeneration, but treatment is available to slow the effects.
Retinal Detachment
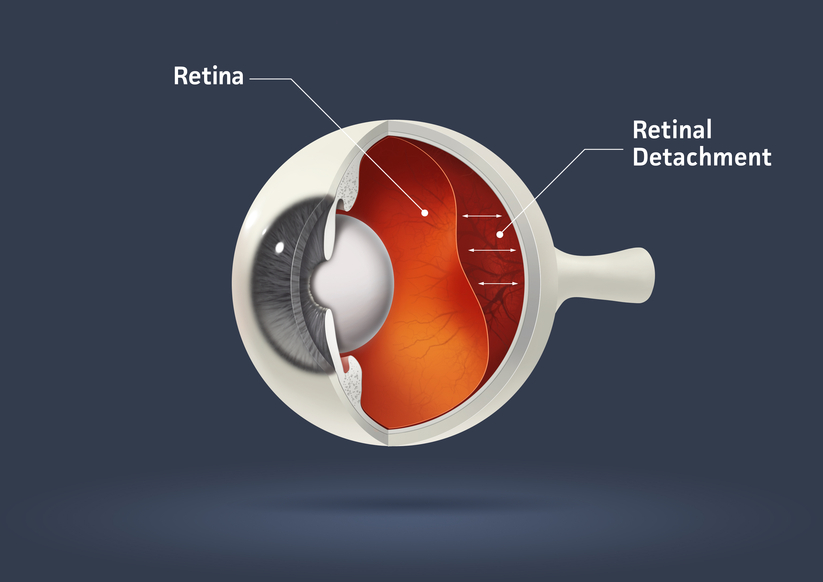
The part of the eye which collects light and transmits the light messages to the optic nerve and brain is the retina. It lines the inner back wall of the eye. When the retina separates from the back wall, it is known as retinal detachment. It is a serious condition which can cause permanent damage and vision loss if not treated quickly.
Symptoms
A retinal detachment often causes sudden defects in your vision. It may just cause a blind spot too small to notice, or it may cause a noticeable shadow which obscures your vision. An increase in “floaters,” which look like small particles or fine threads, may also be noticed. Finally, flashes of light are associated with retinal detachment.
Risk Factors
Eye injuries, tumors, and cataract surgery can cause retinal detachment. Nearsighted individuals and the elderly are at greater risk for spontaneous detachment. Also, diabetic retinopathy, a condition associated with diabetes, can cause bleeding which leads to retinal detachment.
Retinal Toxicity – Hydroxychloroquine
Hydroxychloroquine is an antimalarial drug that also elicits an immunomodulatory effect. Therefore, it is also widely used to treat autoimmune conditions such as rheumatoid arthritis and systemic lupus erythematosus. As an inhibitor of heme polymerase, it is also believed to have additional antiviral activity and has been used as a short-term treatment for the coronavirus pandemic.
While rare, long-term use of hydroxychloroquine, also known as Plaquenil™ can cause toxicity to the macula based on one’s cumulative lifetime dose. Toxicity and vision loss can be minimized with proper dosing and monitoring. Consequently, it is important for those on the drug to understand that just because no macular toxicity is found this year, there still could be problems next year.
Macular toxicity
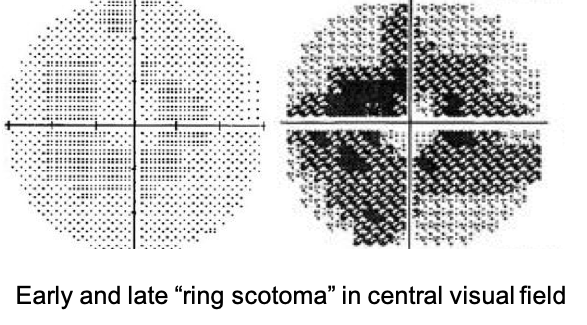 For the most part, toxicity will not begin until one has been on the drug for five years. When starting on hydroxychloroquine, it is important to get a baseline eye exam, with repeat examination and testing every year until the fifth year is reached. After five years, testing should take place every six months. Toxicity manifests as a "bull's eye" macular lesion with a corresponding ring-like visual field defect in the central vision. Unfortunately, once these signs are actually visible upon clinical evaluation, the toxicity is already fairly advanced. Therefore, early detection is key to preserving vision.
For the most part, toxicity will not begin until one has been on the drug for five years. When starting on hydroxychloroquine, it is important to get a baseline eye exam, with repeat examination and testing every year until the fifth year is reached. After five years, testing should take place every six months. Toxicity manifests as a "bull's eye" macular lesion with a corresponding ring-like visual field defect in the central vision. Unfortunately, once these signs are actually visible upon clinical evaluation, the toxicity is already fairly advanced. Therefore, early detection is key to preserving vision.
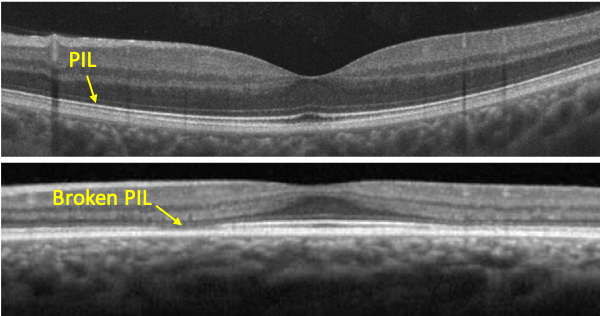 Fortunately, OCT of the macula can detect changes very early. In the diagram, the photoreceptor integrity line (PIL) is noted. This is where the inner and outer segments of the retinal photoreceptors meet. The earliest change noted on OCT is a break in the PIL. If changes on OCT are detected and if Plaquenil is stopped, vision is preserved in most cases. Measurement of the central visual field is also still considered a standard of care and should be performed yearly. However, OCT will likely detect macular toxicity before a visual field defect develops.
Fortunately, OCT of the macula can detect changes very early. In the diagram, the photoreceptor integrity line (PIL) is noted. This is where the inner and outer segments of the retinal photoreceptors meet. The earliest change noted on OCT is a break in the PIL. If changes on OCT are detected and if Plaquenil is stopped, vision is preserved in most cases. Measurement of the central visual field is also still considered a standard of care and should be performed yearly. However, OCT will likely detect macular toxicity before a visual field defect develops.
Weight-based dosing
The key to minimizing the risk of retinal toxicity is appropriate dose based on body weight. Revised guidelines from the American Academy of Ophthalmology (AAO) in 2016 state that to reduce the chance of macular toxicity, the maximum dosage of Plaquenil should be 5 mg/kg of body weight. While typical dosing has been two 200 mg tablets per day, by the revised guidelines, anyone weighing less than 180 lbs. should possibly be taking less.
Patients who take an appropriate dose based on body weight have a less than 1% risk for developing Plaquenil retinal toxicity during the first 5 years of use and less than 2% during the first 10 years of use. The risk rises to nearly 20% after 20 years of use, but a patient who screens as normal after 20 years has only a 4% risk for converting to toxicity in the subsequent year. However, if one’s daily dose is higher than what is appropriate based on body weight, their risk of toxicity increases.
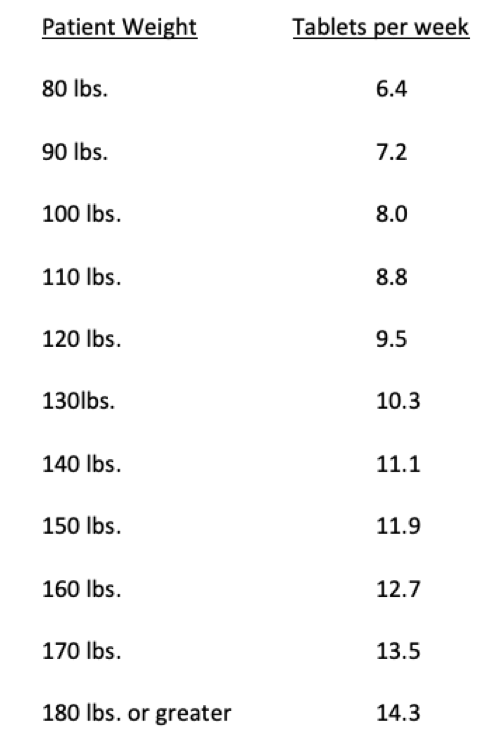 Plaquenil is slow to stabilize in the body, so it does not have to be taken at the same dose each day. As Plaquenil only comes in 200 mg tablets, proper dosing can be achieved by calculating a patient’s daily dose based on their body weight in kilograms, multiplied by 5 mg per day to get their maximum daily dose. Multiply this by 7 for their weekly dose, then divide by 200 to determine the number of tablets to take weekly.
Plaquenil is slow to stabilize in the body, so it does not have to be taken at the same dose each day. As Plaquenil only comes in 200 mg tablets, proper dosing can be achieved by calculating a patient’s daily dose based on their body weight in kilograms, multiplied by 5 mg per day to get their maximum daily dose. Multiply this by 7 for their weekly dose, then divide by 200 to determine the number of tablets to take weekly.
For example, let’s say someone weighs 150 lbs. 150 / 2.2 = 68 kg x 5 mg per day = 340 mg per day maximum dose x 7days = 2,380 mg per week, divided by 200 = 12 tablets per week. So, this patient will take 2 tablets 5 days per week and 1 tablet 2 days per week. In other words, we can have this patient take two tablets per day except for say Wednesday and Saturday when they should take one tablet.
In the table to the left, note that the number of tablets per week is extended to the first decimal point. A physician may decide to round up or down based on one’s clinical picture. However, note that even when rounding up, the prescribed dosage will still be within 1 tablet of AAO guidelines.
Other Considerations
Patients with renal disease are at a higher risk of macular toxicity. Hydroxychloroquine is cleared to a large degree by the kidney, so if the renal system is compromised, this effectively increases the circulating level of the drug. Patients with renal disease can have unpredictably high blood drug levels, so both dosage and ocular screening frequency may need to be adjusted to guard against macular toxicity.
Patients using the drug tamoxifen are at a five times greater risk of developing macular toxicity. Therefore, patients taking tamoxifen require careful dosing and screening.
Please bear in mind that the information in this website is by no means meant to replace the advice of your physician. Dr. Morgan recommends that you always follow the advice of your doctor prescribing your hydroxychloroquine. The information provided herein is strictly meant to educate the reader on the possible ocular side effects of hydroxychloroquine and how they can be mitigated.
Call us today
If you are taking hydroxychloroquine, our office would be happy to monitor your eyes for signs of macular toxicity. Dr Morgan’s goal is to fully explain all findings to you during your exam. Dr. Morgan will then send a detailed report of his exam findings back to your prescribing physician.